
글로벌 연구동향
방사선종양학


- 2022년 05월호
[Cancers (Basel).] Prospective Study of Proton Therapy for Lung Cancer Patients with Poor Lung Function or Pulmonary Fibrosis성균관의대 / 노재명, 유홍석, 표홍렬*
- 출처
- Cancers (Basel).
- 등재일
- 2022 Mar 11
- 저널이슈번호
- 14(6):1445. doi: 10.3390/cancers14061445.
- 내용
Abstract
PBT has a unique depth-dose curve with a Bragg peak that enables one to reduce the dose to normal lung tissue. We prospectively enrolled 54 patients with non-small cell lung cancer treated with definitive PBT. The inclusion criteria were forced expiratory volume in 1 s (FEV1) ≤ 1.0 L or FEV1 ≤ 50% of predicted or diffusing capacity of the lungs for carbon monoxide (DLco) ≤ 50%, or pulmonary fibrosis. The primary endpoint was grade ≥ 3 pulmonary toxicity, and secondary endpoints were changes in pulmonary function and quality of life. The median age was 71.5 years (range, 57-87). Fifteen (27.8%) and fourteen (25.9%) patients had IPF and combined pulmonary fibrosis and emphysema, respectively. The median predicted forced vital capacity (FVC), FEV1, and DLco were 77% (range, 42-104%), 66% (range, 31-117%), and 46% (range, 23-94%), respectively. During the follow-up (median, 14.7 months), seven (13.0%) patients experienced grade ≥ 3 pulmonary toxicity. Seven months after the completion of PBT, patients with IPF or non-IPF interstitial lung disease (ILD) experienced a decrease in the FVC but the decrease in DLco was not significant. Under careful monitoring by pulmonologists, PBT could be a useful treatment modality for lung cancer patients with poor lung function or pulmonary fibrosis.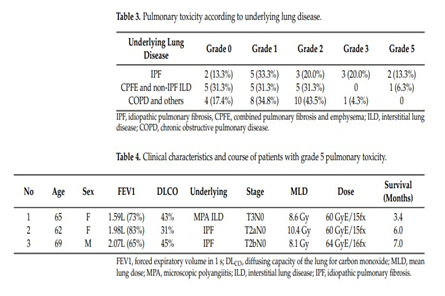
Affiliations
Jae Myoung Noh 1 , Hongseok Yoo 2 , Woojin Lee 1 , Hye Yun Park 2 , Sun Hye Shin 2 , Hongryull Pyo 1
1 Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
2 Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
- 키워드
- idiopathic pulmonary fibrosis; interstitial lung disease; lung cancer; proton beam therapy; radiotherapy.
- 덧글달기


