
글로벌 연구동향
방사선종양학


![[Front Oncol .] Consolidatory ablative stereotactic body radiation therapy after induction chemotherapy for unresectable pancreatic cancer: A single center experience](/enewspaper/upimages/1672981514admin.JPG) 2023년 01월호
2023년 01월호
[Front Oncol .] Consolidatory ablative stereotactic body radiation therapy after induction chemotherapy for unresectable pancreatic cancer: A single center experience서울의대 / 이혜인, 강현철, 지의규*
- 출처
- Front Oncol .
- 등재일
- 2022 Nov 18
- 저널이슈번호
- 12:974454. doi: 10.3389/fonc.2022.974454. eCollection 2022.
- 내용
Abstract
Background and purpose: Consolidatory radiotherapy in form of stereotactic body radiation therapy (SBRT) with an ablative dose following induction chemotherapy is emerging as a promising treatment scheme for unresectable pancreatic cancer. Outcomes of given treatment at a single center for contiguous patients with unresectable pancreatic cancer were evaluated to build the optimal treatment strategy.Materials and methods: In this retrospective study, a total of 50 patients with unresectable pancreatic cancer who underwent induction chemotherapy and ablative dose SBRT were included. SBRT dose was 40-50 Gy in five fractions. Two strategies were adopted to adhere to the organs at risk (OAR) dose constraints: simultaneous integrated protection (SIP) technique and magnetic resonance (MR)-guided adaptive technique. Overall survival (OS) and local progression-free survival (LPFS) were calculated from the start date of SBRT.
Results: The median follow-up period for survivors was 21.1 months (range, 6.2-61.0 months). Eleven (22.0%) patients underwent resection after SBRT, which were all R0 resection. In patients with non-metastatic disease, the median OS was 26.5 months (range, 4.1-61.0 months), and the 1- and 3-year LPFS were 90.0% (95% confidence interval [CI], 72.0-96.7%) and 57.4% (95% CI, 31.7-76.4%), respectively. Patients with oligometastatic disease had inferior survival outcomes, but there was no survival difference among responders to induction chemotherapy. In the multivariable analysis, tumor size ≤4 cm, non-metastatic status, and good response to induction chemotherapy were associated with improved LPFS. In dosimetric analysis, GTV Dmin ≥50.5 Gy was the strongest prognosticator against local progression. Grade ≥3 adverse events occurred in two (4.0%) patients with non-adaptive RT, but none in patients with MR-guided adaptive RT.
Conclusion: Ablative dose SBRT following induction chemotherapy is an effective strategy for selected patients with unresectable pancreatic cancer. The SIP technique and MR-guided adaptive RT were attributed to minimizing the risk of adverse events. Further studies are needed to identify the best candidates for consolidatory SBRT in unresectable pancreatic cancer.
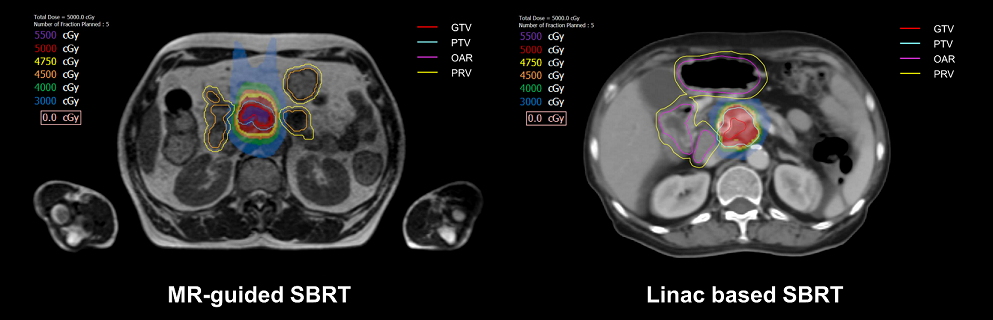
fig1.
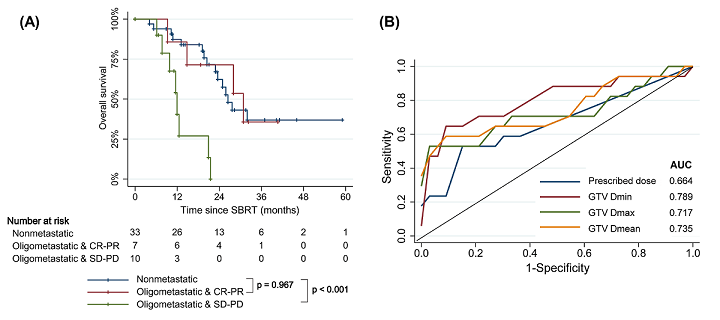
fig2
Affiliations
Hye In Lee 1 2, Hyun-Cheol Kang 1 2, Eui Kyu Chie 1 2 3
1Department of Radiation Oncology, Seoul National University College of Medicine, Seoul, South Korea.
2Department of Radiation Oncology, Seoul National University Hospital, Seoul, South Korea.
3Institute of Radiation Medicine, Medical Research Center, Seoul National University, Seoul, South Korea.
- 키워드
- MR-guided adaptive radiotherapy; ablative dose; oligometastatic disease; pancreatic cancer; simultaneous integrated protection; stereotactic body radiotherapy.
- 연구소개
- 본 연구는 절제 불가능한 췌장암 환자들을 대상으로 시행한 단일기관 후향적 연구입니다. 2017년부터 2021년까지 총 50명의 절제 불가능한 췌장암 환자에서 40 Gy 이상의 ablative dose SBRT를 시행한 결과, median survival 26.5개월, 1-year survival 90%, Grade ≥3 toxicity 4%의 우수한 성적을 확인하였습니다. 이는 MR-guided RT 및 SIP technique을 이용하여 정상 장기를 보호하면서도 동시에 췌장암에 높은 선량을 조사할 수 있었기 때문으로 생각됩니다. 특히 GTV Dmin을 50.5Gy 이상으로 하는 것이 우수한 국소제어율과 가장 연관되었습니다. 췌장암 환자들 중 종양 크기 4cm 이하, 원격전이가 없는 환자, induction chemotherapy에 반응이 좋았던 환자들이 ablative dose SBRT 이후 가장 우수한 성적을 보였습니다. 뿐만 아니라 oligo-metastatic 환자들 중에서도 induction chemotherapy에 좋은 반응을 보이는 경우 우수한 국소제어율이 관찰되어, 이들 역시 ablative dose SBRT candidate로서 가능성을 보였습니다.
- 덧글달기
- 이전글 [Radiother Oncol .] A phase II trial of hypofractionated high-dose proton beam therapy for unresectable liver metastases
- 다음글 [J Cancer Res Clin Oncol .] Application of real-time MRI-guided linear accelerator in stereotactic ablative body radiotherapy for non-small cell lung cancer: one step forward to precise targeting



편집위원
절제불가능 췌장암에서 선행항암화학요법 후 MRI 유도 방사선치료 혹은 SIP (simultaneous integrated protection) 기법을 이용하여 손상위험장기에 대한 선량제한을 맞추어 체부정위방사선치료를 시행한 치료성적을 분석하였음. SIP 기법을 이용한 환자의 8.3%에서 3등급 독성이 발생하였고, MRI 유도 방사선치료를 시행한 환자에서는 3등급 독성은 없었음.
덧글달기닫기2023-01-06 14:49:06
등록