
글로벌 연구동향
방사선종양학


![[Int J Radiat Oncol Biol Phys.] Risk of Hypothyroidism in Women After Radiation Therapy for Breast Cancer](/enewspaper/upimages/1627980800admin.JPG) 2021년 08월호
2021년 08월호
[Int J Radiat Oncol Biol Phys.] Risk of Hypothyroidism in Women After Radiation Therapy for Breast Cancer 유방암 방사선치료 후 갑상선저하증 위험도연세의대 / 최서희, 장지석*
- 출처
- Int J Radiat Oncol Biol Phys.
- 등재일
- 2021 Jun 1
- 저널이슈번호
- 110(2):462-472. doi: 10.1016/j.ijrobp.2020.12.047.
- 내용
-
Abstract
Purpose: To study the hypothyroidism risk after adjuvant radiation therapy (RT) and the association of different RT targets with hypothyroidism risk.Methods: We studied 4073 women treated with adjuvant RT for breast cancer from 2007 to 2016. The primary endpoint was hypothyroidism development after RT. Patients were divided and analyzed into 3 groups: whole breast (WB)-alone (n = 2468), regional node irradiation (RNI)-Lv.4 (n = 215; cranial border at the subclavian artery, according to the European Society for Radiotherapy and Oncology consensus guideline), and RNI-supraclavicular lymph node (SCL) (n = 1390; cranial border at the cricoid cartilage). In general, RNI-Lv.4 was used in the patients with high-risk pN0 and pN1 breast cancer. In auxiliary analysis, the mean thyroid dose was estimated in each group (total n = 600, 200 from each group). All the doses were converted to the equivalent dose in 2 Gy fractions (EQD2) with α/β ratios of 3.
Results: The median follow-up duration was 84 months (WB-alone, 84 months; RNI-Lv.4, 44 months; RNI-SCL, 91 months). The 3-year hypothyroidism incidence rate differed significantly between the RNI-SCL and WB-alone groups (2.2% vs 0.8%; Bonferroni corrected P [Pc] < .001) but not between the RNI-Lv.4 and WB-alone groups (0.9% vs 0.8%; Pc > .05). The Cox model revealed an adjusted hazard ratio of 2.25 (95% CI, 1.49-3.38) for RNI-SCL vs WB-alone, 1.69 (95% CI, 1.12-2.56) for adjuvant systemic therapies, and 2.07 (95% CI, 1.07-3.99) for age <60 years. In the subgroup analysis, the hypothyroidism risk became more prominent in patients aged <60 years. The mean exposure doses to the thyroid were 0.23 versus 1.93 versus 7.89 Gy (EQD2) for the WB-alone versus RNI-Lv.4 versus RNI-SCL groups (P < .001). No statistically different locoregional recurrence rates were seen between groups (5-year rate: <3%).
Conclusions: The risk of hypothyroidism increases after RNI-SCL for breast cancer but not after RNI-Lv 4. These data support routine contouring of the thyroid in the RNI setting, and future studies are required to develop optimal dose-volume constraints.

그림 (1): 세 그룹에서 방사선 조사범위의 차이
세 그룹에서 방사선 조사범위 비교 예시
(A) 유방단독조사군(WB RT alone): 전체 유방 범위만 포함되고 상부 림프절 범위는 포함되지 않아, 갑상선에 조사되는 방사선량이 적음
(B) 제한범위 림프절 방사선조사군 (RNI-Lv.4): 쇄골 상부 림프절 영역 방사선조사범위에 포함되지만, 위쪽 경계가 쇄골 상부 동맥에 국한됨
(C) 전체쇄골상부림프절 방사선조사군 (RNI-SCL): 쇄골 상부 림프절 영역이 모두 조사범위에 포함되어 방사선에 조사되는 방사선량이 많음
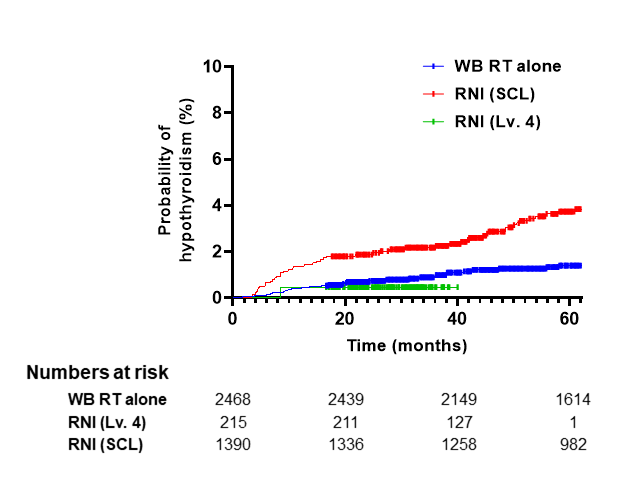
그림 (2): 방사선조사 범위에 따라 나눈 3그룹 각각에서 갑상선기능저하증 발생 확률
유방단독조사군(WB RT alone)과 제한범위 림프절 방사선조사군 (RNI-Lv.4)간 유의한 차이는 없었으나 전체쇄골상부림프절 방사선조사군 (RNI-SCL)에서 갑상선기능저하증의 유의한 증가를 보였음. 3년 후 갑상선기능저하증 발생확률은 WB RT alone군, RNI-Lv.4군, RNI-SCL군에서 각각 0.8%, 0.9%, 2.2% 였음.
Affiliations
Seo Hee Choi 1 , Jee Suk Chang 2 , Hwa Kyung Byun 3 , Nak-Hoon Son 3 , Chae-Seon Hong 1 , Namki Hong 4 , Ye-In Park Ms 1 , Jihun Kim 5 , Jin Sung Kim 5 , Yong Bae Kim 5
1 Department of Radiation Oncology, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Gyeonggi-do, Republic of Korea.
2 Department of Radiation Oncology, Yonsei University College of Medicine, Seoul, Korea. Electronic address: changjeesuk@yuhs.ac.
3 Data Science Team, Center for Digital Health, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Gyeonggi-do, Republic of Korea.
4 Department of Internal Medicine, Endocrine Research Institute, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
5 Department of Radiation Oncology, Yonsei University College of Medicine, Seoul, Korea.
- 연구소개
- 본 연구는 2007년부터 2016년까지 연세암병원에서 유방암 수술 후 방사선치료를 받은 환자 4073명에서 방사선 조사범위와 갑상선기능저하증 발생률 간 관련성을 분석한 연구입니다. 연세암병원에서는 각 환자의 림프절 전이 확률에 따라 쇄골 상부 림프절 (supraclavicular lymph node)조사 범위가 크게 다음의 3가지 (유방만 조사(“WB RT alone”), 미국방사선종양학회(RTOG) 가이드라인에 따라 전체 쇄골 상부 영역 조사(“RNI-SCL”), 유럽방사선종양학회(ESTRO) 가이드라인에 따라 level 4에 국한된 영역만 조사(“RNI-Lv.4”))으로 나뉘었었습니다. 최근 발표된 ESTRO 가이드라인에서는 저위험군 환자에서는 전체 쇄골 상부 림프절에 방사선을 조사하는 것보다 작은 범위(위 경계: 쇄골하동맥까지의)만 조사할 것을 권고하고 있습니다. 분석 결과, 실제 쇄골 상부 림프절 조사 범위가 넓어질수록 인접한 갑상선에 미치는 영향이 늘어나 갑상선기능저하증 발생이 유의하게 증가함을 확인하였습니다. 또한, 갑상선 조사선량이 평균 2 Gy이상일 때 갑상선기능저하증 발생이 유의하게 증가함을 발견해, 임상에서 적용할 수 있는 실질적 제한 선량을 제시할 수 있었습니다. 본 연구는 그간 연구가 부족해왔던 유방암 방사선치료와 갑상선기능의 관련성에 대해, 대규모 데이터와 방사선량학적 정보를 활용하여 결론을 얻은 연구입니다. 특히 정밀 방사선치료시대에, 부작용은 최소화하면서 치료 효과는 극대화 시킬 수 있도록 환자별 최적의 방사선 조사 범위를 결정해야한다는 큰 시사점을 주는 연구라 할 수 있습니다.
- 덧글달기



편집위원
유방암 방사선치료 후 영역림프절 치료여부 및 그 범위에 따라 갑상선기능저하증의 위험도를 분석한 논문으로, subclavian a.까지만 Lv4를 포함한 경우(0.8% at 3yr)에는 전유방방사선치료(0.9%)와 차이가 없었고, cricoid cartilage까지 포함한 경우(2.2%)는 유의하게 발생률이 높음.
덧글달기닫기2021-07-27 14:30:56
등록
편집위원2
두경부암이나 림프종과 달리 유방암에서 regional lymph node irradiation시 hypothyroidism risk가 잘 알려지지 않았는데, 비록 후향적 연구이기는 하지만 단일기관에서 많은 환자를 대상으로 쇄골상부림프절을 포함하여 방사선치료를 시행하면 hypothyroidism 발생 위험이 증가한다는 연구결과는 방사선치료 계획 및 부작용 예측에 도움이 될 것으로 생각됩니다.
덧글달기닫기2021-07-27 14:34:59
등록